Tonight the President will deliver a critical Speech on Health Care to a joint sessions of Congress, and in it he will outline exactly what it is he expects Congress to deliver to his desk. It's expected to be a speech that will either make or break his Health Care Plan.
But I have an answer of my own.
Of course, before you can answer any question (like say "42"), you have to fully understand what the question is.
And in this case the real question is: What can Congress ultimately deliver to his desk when the progressive caucus demands access to a Public Health Care Option and the various Blue Dogs refuse to even consider it?
How about the Best of Both Worlds, the Public Option of Buying into Medicare if and when the Private Insurance Companies Fail to Perform. This I consider a Win/Win Scenario because if they do perform, we Win, and if they don't - We Sill Win.
As things currently stand we have 5 different Health Care Bills in Congress. 4 out of 5 (3 in the House and 1 in the Senate) include a Public Not-For-Profit Health Insurance Option which would be paid for by the premiums of it's members. One Bill from the Senate Finance Committee does not and instead offers some form of Non-Profit Co-ops as an option.
No Bill Currently includes Triggers, or even defines what a Trigger might look like - which leaves open a window of opportunity for us, the progressives, to define what an acceptable trigger might be and how short the time frame for it could have.
Most of the Bills are similar in that they all include a new Nation-Wide Health Care Exchange modeled on the Federal Employees Benefits Program which allows the leveraging of 10 Million Health Consumers to pool and leverage their buying power and keep costs down by purchasing in bulk.
If any of these plans pass, about 250 Million Americans would gain that type of buying power.
All of these plans ban the use of preexisting conditions to block access to care, and the preemptive canceling of care and claims simply because people get sick. Most Insurance Agencies currently spend about 20% of their overhead attempting to find ways to cancel coverage or claims, and has recently been shown by the California Nurses Association an average of about 30% of claim are denied using this tactic. All of the plans in addition to these reforms include some methodology to subsidize those with low-incomes, or those who are either unemployed or their employer refuses to provide Health Care Options for them.
There remains just one major bone of contention, should an additional Not-For-Profit Option be included as part of the Health Exchange and what would that plan look like?
Many different ideas have been debated from Medicare-For-All, a brand new Insurance Plan similar to Medicare Part A with it's own independent Trust Fund or some type of Public/Private Member Owned Co-operative?
The last issue has been whether such an Option should be available on Day One of Year One of the plan, or that it should kick-in automatically in subsequent years if Private Insurance Companies fail to meet certain criteria.
No More Death by Spreadsheet.
With Pre-Existing Conditions and unjustified claim-denials off the table, with a Health Exchange that will allow the type of Interstate Access to Care even Republicans like Mike Pence in the mix - there really isn't much more we can expect out of the Private Companies except better prices.
Some have said that using the Public Option as a loaded gun pointed at the Heads of the Insurance State, ready to fire at will - simply isn't enough.
Or is it?
As I posted a few days ago, there was a period in time when rate of Medical Inflation actually came back down to Earth - and it didn't take a Public Option to do it. All it took was the Threat of one.
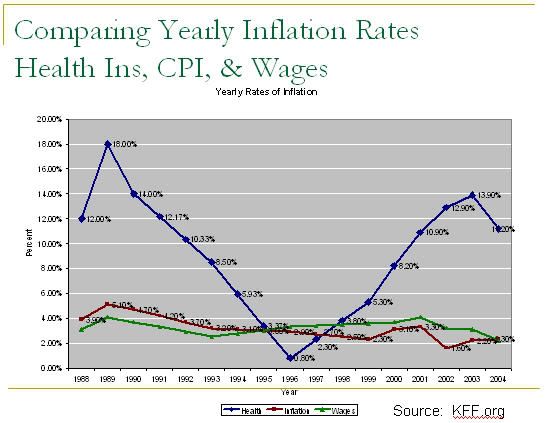
In 1996 in the aftermath of the Clinton Era Health Care effort - and within 3 Years of it's initiation - the rate of increase for the cost of Health Care actually dropped below both the Consumer Price Index and the rate of Wage Inflation.
That Should be the Trigger Point.
If within one year of Day One, the Health Insurance Agencies can not repeat what they've previously done and bring costs down significantly - and keep them down - to levels matching or surpassing the CPI and WI the people of that state automatically are allowed to Buy-in to Medicare as an additional Option in their Health Exchange.
If prices begin to rise again in the future, as they did in the late 90's - the Trigger remains Operational and call be pulled at ANY TIME conditions are met.
Five Years, as Bob Dole has suggested, is too long and frankly unnecessary - the Industry has already shown it can move far more rapidly than that when it has incentive to do so.
Some say we shouldn't have to wait a year or two, that we need this NOW - but let's be realistic - a completely new Public Insurance Plan would take at least 2-3 Years to get up on it's feet and running. It would have to be Staffed. it would have to setup facilities and operational instructions. People would have to be trained. It would have to be FUNDED! No matter which way we go - no Option is going to be implemented immediately. So if we have to wait no matter what, we might as well have Medicare at the end of the rainbow waiting for us. It's already staffed, it's already funded - it's ready to go. Medicare would also have the necessary heft to positively impact the Market that the smaller weaker Co-Ops would lack, but would retain the trust of the American people as a system they can rely on.
All we have to do is Pull The Trigger.
I have stated before that I have some concerns with opening up Medicare because of the projected insolvency of it's trust fund, versus establishing an entirely new Public Plan with it's own fund. I still have that concern but it can be tempered. Part of the funds problem relates to the demographics of more an more Baby-Boomers entering the program and using it's services while fewer and fewer young people are paying into the system. Having younger people who would need fewer services buy-in to the fund would help shore it up considerably.
The one immediate benefit, besides saving on the start-up cost and time required for a brand new system is the fact that Medicare is something that people understand and trust. If we tell the screamers we're going to let their kids buy Medicare if they want, I don't think they'll have much left to scream about. (Even though we all know they still find something out in the fever swamp of WND to complain about) Another is the fact that the Savings would be immediate as I've posted before the costs of America current Public Health System (Medicare/Medicaid/VA/Tricare) is significantly less than it's Private System, particularly when compared to costs internationally.
Via the UN.
| HDI Rank | Expenditure on health (% of GDP) | Public | Private | Combined |
| 12 | United States | 6.9 | 8.5 | 15.4 |
| 106 | Occupied Palestinian Territories | 7.8 | 5.2 | 13 |
| 164 | Malawi | 9.6 | 3.2 | 12.9 |
| 88 | Lebanon | 3.2 | 8.4 | 11.6 |
| 7 | Switzerland | 6.7 | 4.8 | 11.5 |
| 123 | Sao Tome and Principe | 9.9 | 1.6 | 11.5 |
| 150 | Timor-Leste | 8.8 | 2.4 | 11.2 |
| 22 | Germany | 8.2 | 2.4 | 10.6 |
| 10 | France | 8.2 | 2.3 | 10.5 |
| 15 | Austria | 7.8 | 2.5 | 10.3 |
| 1 | Iceland | 8.3 | 1.6 | 9.9 |
| 4 | Canada | 6.8 | 3 | 9.8 |
| 29 | Portugal | 7 | 2.8 | 9.8 |
| 86 | Jordan | 4.7 | 5.1 | 9.8 |
| 2 | Norway | 8.1 | 1.6 | 9.7 |
| 13 | Spain | 5.7 | 2.4 | 8.1 |
| 16 | United Kingdom | 7 | 1.1 | 8.1 |
On a per capita basis the U.S. currently spends (nearly) twice as much as
(Top UN Ranked Countries by Human Development Index with Per Capital Health Care Expenses 2004)
| 1 Iceland | 3,294 |
| 2 Norway | $4,080 |
| 3 Australia | $3,123 |
| 4 Canada | $3,173 |
| 5 Ireland | $2,618 |
| 6 Sweden | $2,828 |
| 7 Switzerland | $4,011 |
| 8 Japan | $2,293 |
| 9 Netherlands | $3,092 |
| 10 France | $3,040 |
| 11 Finland | $2,203 |
| 12 United States | $6,096 |
The other part of the issue is yet again, the completely out-of-whack rate of Medical Inflation in the U.S. If we do manage to bring that Inflation Rate down, we improve the solvency of the Trust Fund - so this plan has a two-fer effect of helping to bring overall costs down for everyone and effectively Saving Medicare for the forseeable future.
Medicare isn't perfect, some doctors refuse to accept it because it pays less, and it still has problem with prescription drugs in Part D with the Big Fat Donut Hole and inability to bargain for better prices.
Still, this plan has the benefit that it might be something that both Anthony Weiner and Olympia Snowe could sign on to. Both Ben Nelson and Joe Lieberman oppose the Public Option but have gone on record that they could support it with a Trigger. Rather than further compromise and deal away the P.O. we should make hem ante-up - you get a trigger if we get Medicare for anyone willing to buy-in to it. We could have Everything We Want. How could those who've argued for a Co-Op say no to a Medicare Buy-in as an alternative? We could even toss in some token Tort Reform and Medical Savings Accounts as a sweetener and anything is possible - even significant serious Health Care Reform in our Lifetime.
I'm sure Barack Obama will deliver a barn-burner of a Speech Tonight, but when it's all over - I strongly suspect what comes out of Congress will look a lot like what I've just described here.
Vyan
No comments:
Post a Comment